I just want to share this article from dr. Sam Bailey on this blog, in continuation to previous articles about "Virus mythology"
THE MONKEYPOX MYTHOLOGY
link:https://drsambailey.com/viruses/monkeypox-mythology/
link video:
https://odysee.com/Monkeypox-VIDEO-1080p:7f5f3bcd69d8a8bd8214a31a21217272a4527b85

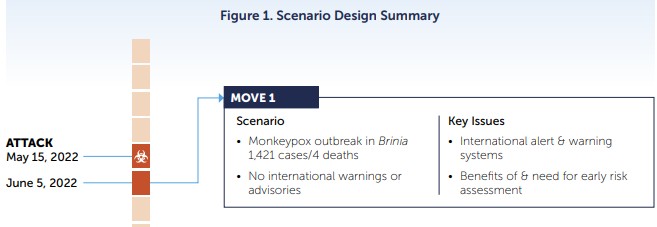
“Monkeypox” – who could have seen it coming? Well, apparently the organisation founded by Ted Turner in 2001 called the ‘Nuclear Threat Initiative’ (NTI) saw it coming when they published a report in November 2021 called, “Strengthening Global Systems to Prevent and Respond to High-Consequence Biological Threats.” The report states that in March 2021, they partnered with the Munich Security Conference to run an exercise scenario involving a, “deadly, global pandemic involving an unusual strain of monkeypox virus that emerged in the fictional nation of Brinia and spread globally over 18 months…the fictional pandemic resulted in more than three billion cases and 270 million fatalities worldwide.”

Amazingly, the scenario had the monkeypox outbreak emerging as a result of an act of bioterrorism in May 2022, right where we are now. We have dealt with gain of function garbage involving non-existent viruses in several other videos, while Dr Stefan Lanka has also dismantled such fallacies. Regardless, the NTI’s report suggests that what is required in a fantasy outbreak is, “aggressive measures to slow virus transmission by shutting down mass gatherings, imposing social-distancing measures, and implementing mask mandates.” The winning countries in the NTI’s hallucination implemented, “large-scale testing and contact-tracing operations and scaled-up their health care systems.”

Their charts, which seem to be produced by Neil Ferguson’s calculator, show that countries that don’t comply with their restrictions and medical interventions will be far worse off. The report goes on to state, “both the exercise scenario and the COVID-19 response demonstrate that early actions by national governments have significant, positive impacts in managing the impact of the disease.” When they say “positive impacts” it is not quite clear who is on the receiving end, although they note that “the COVID vaccine market will exceed $150 billion in 2021.” All in all the NTI’s report reads like Event 201 on Ritalin. (Event 201 took place on 18 October, 2019. It was an exercise involving a, “coronavirus pandemic” just months before the COVID-19 “pandemic” was declared.)
As with COVID-19 it appears that other parties have also been eagerly awaiting a market such a “pandemic” would present. Likewise, these fortune-tellers were preparing vaccines to go where no vaccine had gone before. In this case the biotech company Bavarian Nordic gained approval from the FDA in 2019 to market JYNNEOS, a smallpox and monkeypox vaccine. Other health authorities were also primed to react to a previously rare condition that has been of no concern for their nations…until now apparently. For example, on May 20, 2022, the UK Health Security Agency published a document titled, “Recommendations for the use of pre and post exposure vaccination during a monkeypox incident.” Like COVID-19, it’s starting to feel like all roads lead to vaccines again…

So now that the scene has been set we can get into the “science” of monkeypox starting with an official description of the alleged viral disease. The CDC states that, “Monkeypox was first discovered in 1958 when two outbreaks of a pox-like disease occurred in colonies of monkeys kept for research, hence the name ‘monkeypox.’ The first human case of monkeypox was recorded in 1970 in the Democratic Republic of Congo.” They go on to state that, “in humans, the symptoms of monkeypox are similar to but milder than the symptoms of smallpox.” The illness is said to be flu-like with the addition of lymph node swelling and then development of a rash, and then lesions that progress from macules to vesicles to scabs.
In terms of the lethality of monkeypox, the CDC state that, “in Africa, monkeypox has been shown to cause death in as many as 1 in 10 persons who contract the disease.” This 10% fatality rate has already stoked the fear narrative and was also used as the case fatality rate in the NTI’s monkeypox pipe dream. It should be noted that historically monkeypox has been virtually unheard of in first world countries and the rare cases are usually in people that have recently arrived from Africa.
Indeed, one of the only recorded “outbreaks” of monkeypox in the first world was in the United States in April 2003. Cases were declared in 6 states and said to be caused by rodents that were imported to Texas from Ghana. This was the first time monkeypox had been reported outside of Africa and the CDC published a paper in 2006 analysing the incident. The paper states that, “person-to-person spread of the virus is thought to occur principally via infectious oropharyngeal exudates” although it is clear that this has never been scientifically established. They continue to say that, “the virus is thought to have been transmitted from African animals” – in other words, it’s another species-jumping pathogen tale.

They reported that, “individuals who had illness onset within 21 days after exposure to MPXV [Monkeypox virus] who experienced fever (defined as a body temperature greater 37.4°C) and vesicular pustular rash or rash (potentially uncharacterized) plus orthopox IgM antibodies were classified as having probable cases of infection.” Now 37.4°C is not a fever in our book, it is a normal body temperature and we would suggest 37.6°C and above qualifies as a fever. We noted in their chart that they were using the classification ≥39.4°C, but this appears to be an error as in another paper, we’ll get to soon, it was once again 37.4°C. The second paper even said the “fever” could be subjective, so they appear to be using this loose criteria and pathologising a normal state. Additionally, the CDC’s weekly report from the 11th of July 2003, stated that from a total of 71 cases, only “two patients, both children, had serious clinical illness; both of these patients have recovered.” The remainder had a variety of respiratory and gastrointestinal symptoms.
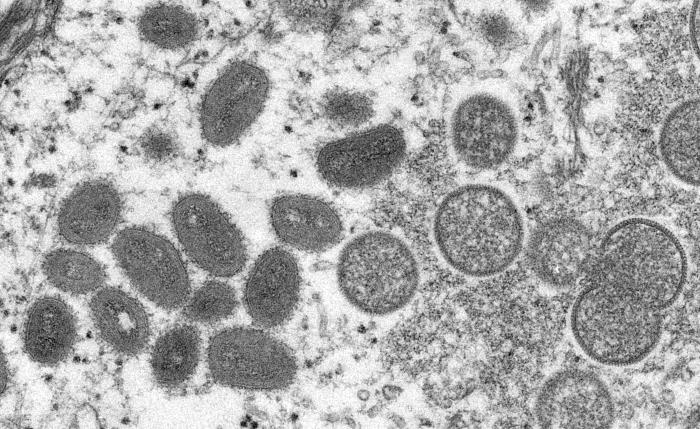
The CDC’s cases were confirmed on the basis of specimens that showed, “monkeypox virus isolation, detection of monkeypox-specific nucleic acid signatures, positive electron-microscopy findings, or positive immunohistochemical findings.” We had a look at the electron micrographs presented by the CDC including the image shown below of a skin sample from one of the patients. The caption informs us that the round particles on the right are immature monkeypox virions, while the oval particles on the left are mature viruses. However, all they have is a static image of dead tissue and no conclusions can be made about the biological role of the imaged particles. None of them have been shown to be replication-competent disease-causing intracellular parasites and so should not be called ‘viruses’.
Looking at the CDC’s weekly report from 2003 again, it appears that the 35 “laboratory-confirmed cases” all involved polymerase chain reaction (PCR) “tests”, so we investigated the scientific evidence behind this claim. One of the citations for the development of PCR detection of monkeypox is a 2004 paper titled “Real-Time PCR System for Detection of Orthopoxviruses and Simultaneous Identification of Smallpox Virus.” Now a PCR protocol requires them to know the genetic sequences of the alleged monkeypox virus, which takes us to this 2001 paper titled, “Human monkeypox and smallpox viruses: genomic comparison”. The paper claimed to have “isolated” the monkeypox virus in a rhesus monkey kidney cell culture from a scab of a monkeypox patient. Here the virologists are up to their old tricks again by asserting that: (a) the patient’s scab contains the monkeypox virus, and (b) it is now in their culture brew. They claimed to have sequenced the “viral genome” by referring to a process described for sequencing an alleged variola virus in 1993.
But when we look at this paper there is no virus demonstrated either, simply an assertion that it was “isolated” from, “the material from a patient from India” in 1967. They go on to make the claim that, “the virions were purified by differential centrifugation and viral DNA was isolated” – however, there is no demonstration of what they purified or how they were determined to be virions. In none of these experiments did they perform any controls by seeing what sequences can be detected from other human-derived scabs or similar specimens from unwell individuals. This is where we need to remind the virologists of what a virus is supposed to be – that is, a replication-competent intracellular parasite that infects and causes disease in a host. It is not detecting genetic sequences contained within scabs and claiming that they belong to a virus.
So returning to the CDC’s paper describing the 2003 “outbreak”, it is unclear how they established they could be diagnosing anyone with monkeypox by using the PCR. Their PCR can only have been calibrated to sequences of unproven provenance. Additionally, it doesn’t matter what kind of analytical specificity their PCR protocol had, there was no established diagnostic specificity – in other words it was not a clinically-validated test, an issue that goes beyond whether the “virus” exists or not. (From the MIQE Guidelines: Analytical specificity refers to the qPCR assay detecting the appropriate target sequence rather than other, nonspecific targets also present in a sample. Diagnostic specificity is the percentage of individuals without a given condition whom the assay identifies as negative for that condition.)
The 47 US cases they ended up describing were all in some sort of contact with imported African prairie dogs and the CDC’s paper concludes that, “individuals contracted MPXV infections from infected prairie dogs; no human-to-human transmission was documented, but there were many different potential scenarios of infection involving respiratory and/or muco-cutaneous exposures, percutaneous and/or inoculation exposures.” Now there were some problems with the study design which they admitted to including that, “the analyses were limited by incomplete reporting or recall of information by patients. And, because of the retrospective nature of the study, we were unable to obtain highly detailed data.”
However, even allowing some wriggle room for them here, the inconsistencies go further still. Firstly, no one in the US incident died from the disease which is said to have a 10% fatality rate in Africa. No doubt, the inconsistent lethality rates will be attributed to different “variants”, but there can’t be variants of something that doesn’t exist.
There were few images available of the skin lesions that were reported in the 2003 incident but two of the US cases are depicted below and an image from a monkeypox case in Africa is shown for comparison. The reader can make up their own mind but those skin reactions do not look remotely comparable to us.



Next, the CDC claim that, “the natural reservoir of monkeypox remains unknown. However, African rodents and non-human primates (like monkeys) may harbor the virus and infect people” – in other words it’s all rather vague and remains an unproven hypothesis. Now, obviously some people became unwell in the US in 2003 but with the viral theory we are supposed to believe that it jumped from some prairie dogs to some humans and the latter became infected with the alleged virus…but then no human could pass it on to another human. The theory falls flat – a virus needs to spread, if it can’t spread, it’s dead and thus it’s not a virus. And the historical patterns of alleged monkeypox virus outbreaks make no sense – why did it pass to these people so easily and yet it can go a decade between alleged “outbreaks”?
Unfortunately, the 2003 incident was investigated as though the viral contagion theory had already been established and other explanations were ignored. If people were allegedly getting sick from these African rodents, wouldn’t it be a good idea to check the animals for other toxicities, particularly in their faeces and also for any ticks or parasites? We did note another reference state that with regards to the US cases, “many of the people had initial and satellite lesions on palms, soles, and extremities.” However, according to the CDC, monkeypox usually starts on the face so the clinical picture in the US cases was not consistent with cases that are typically described in Africa.
In any case, a review of the scientific evidence revealed that with regards to monkeypox: (a) there is no evidence of a physical particle that meets the definition of a virus, (b) there is no evidence of anything transmitting between humans, and (c) there is no way to confirm a diagnosis of monkeypox unless you believe in clinically-unvalidated tests such as the PCR kits that have been produced. In other words, if we see a monkeypox “pandemic” that is used as an excuse to role out more globalist terrorism, it will be on the back of another PCR pandemic, not one that has any basis in nature.
For those of you wanting to explore more problems with the various monkeypox claims, Mike Stone of ViroLIEgy has written a couple of interesting commentaries. The first article is, “Was Smallpox Really Eradicated?”, which among other things deals with the convenient emergence of monkeypox while smallpox was apparently being eradicated. The second article is, “Did William Heberden Distinguish Chickenpox From Smallpox in 1767?” This outlines the fact that the pox conditions are not as readily distinguishable from each other as the text books suggest and appear to relate more to the severity of a similar disease process. You can also watch our video, “Chickenpox Parties and Varicella Zoster Virus?” to see why there is no evidence of a virus in that related condition either.
From the perspective of terrain theory it is a fundamental mistake to attribute a person’s illness to a supposed virus, as the subsequent “treatments” don’t address the underlying issues. If someone is unwell, then they are usually deficient in nutrients and need to restore balance, or they have been exposed to environmental toxins and need to help the body detoxify. Wars against alleged pathogens that involve treating everyone the same way with civil rights restrictions and vaccines are certainly not about health. It is good to see more people waking up to the COVID-19 fraud so there is hope that a monkeypox scamdemic, if attempted, will bring even more light to the situation. As always, your best health is in your own hands, not in the hands of a globalist cult and their cronies.
7 Comments